

What is hernia?
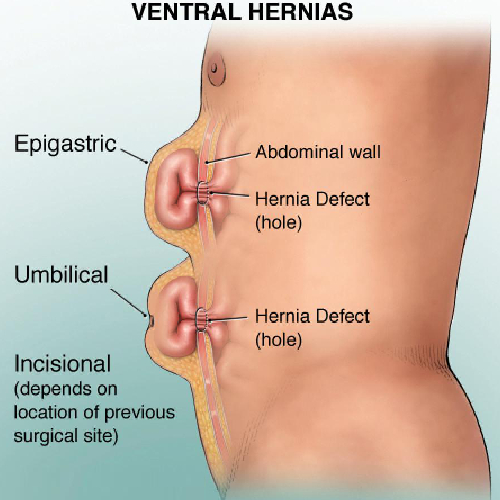
There is a defect or weakening in the muscular or fascial layer of the abdomen, through which abdominal visceral contents like bowel loops or omental fat can protrude out.
Why does hernia occur?
Hernia occurs through naturally weakened areas of the abdomen (Inguinal canal and umbilical tube) or sites of previous surgery and trauma.
Hernia can be congenital (present since birth) or acquired (develop in later age).
Increased abdominal pressure is the main cause of acquired hernia formation.
Factors which contribute to hernia are chronic cough, constipation, urinary symptoms, obesity and smoking.
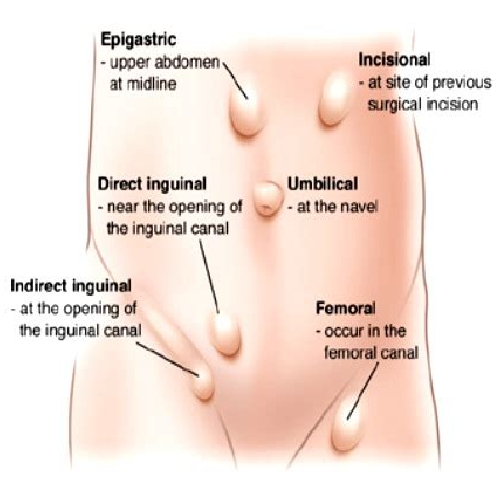
What are common sites of hernia?
They are groin (Inguinal), belly button (Umbilical), upper abdomen (Epigastric) or site of previous operation (Incisional).
What symptoms can occur due to hernia?
Hernia can present solely as a swelling (bulge) beneath the skin, which increases on coughing or straining, and decreases on lying down.
Sometimes people may have dragging sensation, discomfort or pain at the site of bulge.
Continuous pain, redness or tenderness over the swelling, associated with gastro-intestinal symptoms suggests complication of hernia, which warrants urgent surgical intervention.
What is the treatment of choice for hernia?
Hernia never reverses of its own, but gradually keeps on increasing in size over time.
No medicine can treat hernia, as it is a defect in the abdominal wall which need to be repaired surgically.
Use of truss (Hernia belt) is usually ineffective, and only delays the definitive treatment.
Hernia is considered a semi-emergency, requiring early surgery, as it can anytime lead to cascade of complications.
What are the complications which can occur, if hernia is left untreated?
Initially hernia can be reducible, increasing in size on coughing and straining, and decreasing on lying down.
If hernia does not reduce in size on lying down or done manually, it is called irreducible hernia.
Irreducible hernia can further lead to incarcerated, obstructed or strangulated hernia, which is a surgical emergency and can even damage your intestine.
What are the surgical options available?
Hernia can be repaired by open technique or laparoscopically.
Most of the hernias nowadays are repaired laparoscopically. Three to four small punctures are made, varying from 5 – 10 mm in size. Usually performed under General anaesthesia.
Surgical technique:
Inguinal hernias – TEP (Total Extra-peritoneal) or TAPP (Trans-abdominal Pre-Peritoneal) mesh repair
Ventral / Incisional / Umbilical / Epigastric hernias – IPOM (Intra-peritoneal onlay mesh) repair, Hybrid repair or abdominal wall reconstruction.
What are benefits of laparoscopy surgery?
Early recovery after surgery.
Decreased pain.
Better cosmesis. Minimal scar on the abdomen.
Early return to work.
No residual weakness.
Mesh placed posterior to abdominal muscles is superior to anterior mesh placement (Just like tyre puncture, patch put inside is better than putting a patch on outer surface of tyre).
When is laparoscopy surgery not feasible?
Some patients may require open hernia repair in view of large complicated hernias, elderly age or associated co-morbidities where general anaesthesia is contraindicated.
The decision to select type of technique should be left with the surgeon considering the patient’s safety as a priority.
Your surgeon will decide the best method of hernia repair depending on individual situation.
Why a mesh is used to repair a hernia?
Mesh is usually indicated for most of the hernia to do a tension free repair of the hernia defect. Use of mesh decreases the recurrence rate of hernia.
Non-absorbable polypropylene or partially absorbable meshes are used in inguinal hernia repair and abdominal wall reconstruction.
Special composite meshes (prevent mesh complications in contact with abdominal viscera) with fixation devices are used in ventral hernia repair, which adds extra cost to laparoscopy surgery.
What should I expect after surgery?
Usually after laparoscopy surgery, patients can take oral diet and start walking 4 hours after the surgery.
You may expect abdominal discomfort or pain due to mesh placement for initial 24-48 hours, which will be managed using pain-killers.
Discharge is usually planned in 24-48 hours depending on patient comfortability.
With laparoscopic surgery, you will probably be able to get back to your normal activities within a few days. These activities include showering, driving, climbing stairs, lifting, and working.
A follow-up appointment within a week after your operation is scheduled.
Strenuous activity and exercise are restricted for 2 to 4 weeks after surgery.
Is laparoscopy risky for people with other medical problems like Diabetes, Hypertension, Kidney disease or Morbid Obesity?
Not at all. On the contrary, minimization of the trauma to the body by Minimal Access Surgery (MAS) causes minimal disturbance of normal physiology.
Can laparoscopy be performed in children for inguinal hernias?
Yes, laparoscopic herniotomy (mesh is not used) can be safely performed in paediatric population.